 |
 |
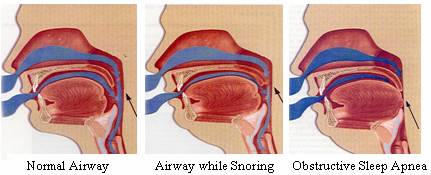
Snoring is a partial blockage of the airway. Complete blockage for several seconds is called obstructive sleep apnea. Untreated Obstructive Sleep Apnea can increase your blood pressure and chances for serious heart problems as much as 50%.
Snoring is a common annoyance affecting 20% of the adult population (25% of adult men). During sleep the muscles of the throat and mouth relax, causing a decrease in the airway spaces. The decreased size causes an increased velocity of air; this causes the soft tissues of the upper airway to vibrate with the resulting noise. An elongated soft palate, enlarged uvula, excessive body weight, heavy alcohol consumption, as well as other sedatives, increase the severity of snoring.
Snoring in and of itself is of no harm to the individual, and may have more significance to those who live with the person snoring than the individual himself. Snoring is significant, however, in that almost all patients with obstructive sleep apnea snore.
Obstructive Sleep Apnea occurs when complete blockage of the airway occurs and the resulting asphyxiation lasts longer than several seconds. Obstructive Sleep Apnea (OSA) is reported in 4% of middle aged men and 2% of middle aged women. The actual numbers may be significantly greater.
The causes of OSA are the same as snoring. Any obstructive condition coupled with assuming the supine position may cause a blockage of the upper airway. The hypoxia (lack of oxygen) resulting from this blockage eventually causes the patient to waken to resume breathing, often with a jump or loud noise.
 |
This sudden awakening may be a total awakening or bringing the sleep level to a lighter level. When this happens throughout the night, the loss of quality sleep results in symptoms such as excessive daytime sleepiness, cognitive dysfunction, memory and judgment impairment, irritability, deceased libido, hypertension, nocturia, sweating, fatigue headaches, depression, and an increased tendency for accidents.
Severe cases of obstructive sleep apnea can cause physical ailments that include: bradycardia (slow heart beat), tachycardia (rapid heart beat), systemic hypertension, pulmonary hypertension, acute pulmonary edema, and reversible high-grade proteinuria. There are multiple paths of treatment for OSA and snoring, all an attempt to keep the airway open when sleeping.
The mandibular repositioning device has statistical evidence supporting its use for both snoring and OSA. Essentially a cousin of the bite plates worn for orthodontics, upper and lower devices hold the lower jaw forward of its natural position. This brings the base of the tongue away from the wall of the pharynx and the airway is opened.The success rate for snoring is in the 75% range, and for mild sleep apnea 50%. Treatment with a mandibular repositioning device is noninvasive and easily accomplished, with a minimal downside if not effective. We can construct one in a few short visits for snoring or OSA problems.
Surgical options include alterations to the nasal passage, soft palate and uvula, shape of the tongue, and location of the upper or lower jaw. The average reduction in OSA is about 50% for most techniques, and about 70% for snoring.
Medications have not, to date, proven effective in preventing OSA.
Nasal Continuous Positive Airway Pressure is a method of providing continuous room air under pressure to patients by using a small air pump connected to a face or nose mask. Used only for OSA, this technique appears to work by splinting the pharyngeal path open creating a more patent airway, thereby reducing swelling due to edema. It is very effective when used for over four hours a night, but patient compliance with the awkward machinery is only 50%.
Behavioral changes, such as changing sleep positions, head posture, quitting smoking, and avoidance of central nervous system depressants may be helpful for some people. Loss of weight in heavier people may increase the size of the airway by reducing the size of the tongue and soft palate.
Each individual presents his own set of causative agents for snoring and/or obstructive sleep apnea. The best treatment for each person must be determined based on the observable problems. Treatment with a mandibular repositioning device is not invasive, easily accomplished, and available as either complete therapy or an adjunct to another form of therapy.
If you have any questions regarding repositioning therapy for snoring or obstructive sleep apnea, please feel free to contact me.
Dentures | Extreme Makeovers | Doctor's Credentials | Map & Policies | Contact Us
Home | Professional Referrals | Tidbits for Dentists | Newsletters for MDs