 |
 |
So, you think you or someone you know has ‘TMJ’. Sooner or later everyone has some pain in the head and neck area. You can’t help hearing or reading about it, every time the media has nothing else to worry you with, this is one of the themes they constantly go back to.
Everyone has a TMJ (Tempromandibular Joint). People who have pain of the head, neck or jaws may well have a dysfunction of the jaw apparatus, but everyone has the joint. If you went to your doctor with a pain in your leg and after, completing an extensive examination, you were told that you have “knee”, it would not be a satisfying diagnosis. Similarly, the symptoms of Tempromandibular Dysfunction (TMD) can not be described by the anatomical location TMJ.
ANATOMY:
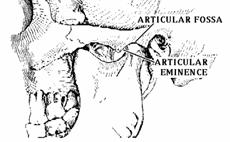
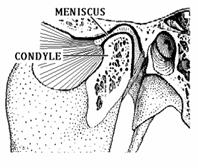
The TMJ is the anatomical joint between the lower jaw (the mandible) and the temporal bone of the skull. If you place your fingers in front of your ears and open your mouth you can probably feel the rounded end of the lower jaw (the condyle) glide forward along the base of the temporal bone (the articular eminence). This joint is the only one of its kind in the body.
Let’s take a close look so you can appreciate the marvel of the TMJ. First it is two joints, one on the right and one on the left, that are rigidly attached via the bone of the mandible so that one can’t move without the other. While they are moving, however, they are not necessarily moving in the same direction or in the same manner. The joints are the only ones in the body that both slide forward and backward (like when you stick your jaw out) and rotate (as in jaw opening). When the teeth are touching, they stop the jaw from sliding forward, so most motions are a combination of both sliding and rotation.
 |
 |
 |
TREATMENT:
Most Tempromandibular Dysfunction is caused by muscle spasm. Simple techniques to reduce tension to the muscles involved will usually reduce the discomfort. Self care practices, for example eating soft foods, applying heat or ice packs, and avoiding extreme jaw movements (such as wide yawning, loud singing or chewing gum) are useful in easing TMD symptoms. Learning special techniques for relaxing or reducing stress may also help patients deal with the pain associated with TMD problems. In addition reversible physical therapy that can be done at home, which focus on gentle muscle stretching and relaxing exercises, as well the use of muscle-relaxants and anti-inflammatory drugs may help the healing process.
During normal function (chewing, swallowing, and speech) the teeth will contact up to 2000 times a day. These contacts are normally light and fleeting. Prolonged contact with excessive force (clenching and grinding the teeth), which is a major cause of TMD, can be greatly reduced by the use of an oral appliance to keep the teeth from contacting. These devices reduce the amount of force that can be produced, and cause different areas of the muscles to function during contact. This is not a life long commitment for most people, but a transient therapy that can always be re-instituted if the problem recurs.
Invasive procedures are usually related to anatomical deformities. These procedures vary from simply changing in the way teeth meet, to surgery on joints with osteoarthritis, and symptomatic disk problems. Few surgical procedures are done today since the criterion for surgery is very limited. So, multiple opinions should be received prior to any surgical procedure for TMD.
What ever the treatment modality, the sooner it is initiated the sooner relief of symptoms can be accomplished. The more muscle damage that occurs the longer the recovery time. It is simple matter to come in, have an evaluation, and be shown the path toward comfort.
Dentures | Extreme Makeovers | Doctor's Credentials | Map & Policies | Contact Us
Home | Professional Referrals | Tidbits for Dentists | Newsletters for MDs